The frenulum of the tongue is a piece of tissue that connects the lower side of the tongue to the bottom of the mouth. Frenulum’s can vary in many ways; they can be short or long, thick wiry or thin membranous, they can end in the middle of the tongue or all the way at the tip. If the frenulum is very short, the mobility of the tongue is limited and this can cause problems when drinking from the breast. At a later age, a short frenulum can cause trouble with for example playing a wind instrument, licking ice cream, kissing or speaking. Whether the too short frenulum will be a relevant problem during breastfeeding differs per baby.
Tongue-tie can be recognized by
- Unable to stick out the tongue far enough (no further than the lower jaw)
- Unable to bring the tongue upwards
- Unable to move the tongue to the sides (left and right)
- Unable to curl the tongue around the base of the nipple and nipple itself
Often the tongue is heart shaped, easily visible when the baby is crying. You usually see more family members with tongue-tie.
Possible problems with breastfeeding due to tongue-tie
- Unable to create a vacuum when latching to the breast
- Unable to hold the vacuum during the sucking which is recognized by the smacking/clucking sounds, restlessness and frustration of the baby
- Bowel cramps, burping and/or reflux (backflow)
- Difficulties with drinking sufficiently from the breast, resulting in extra and often longer feeding sessions
- Drinking is too exhausting for the baby causing it to fall asleep quickly
Consequences
- Not completely emptying the breasts can have a negative effect on the milk production
- The risk of insufficient growth and weight loss due to inadequate milk intake
- It can lead to abrasions and cracks on the nipple, because the nipple is not consistently in the same position during feeding
- Higher chance of blocked lactiferous ducts or inflammations in the breasts because the breasts are not completely emptied, and because of the cracks in the nipple.
The above-mentioned can lead to fatigue and frustration of the mother as well as the baby. Time is needed to figure out the cause, and it also takes time to solve the problem. Finally, the baby must regain confidence in breastfeeding. As soon as the baby discovers that drinking from the breast is pleasurable, the worst of it is usually over.
Cutting/Splitting of the frenulum (frenotomy)
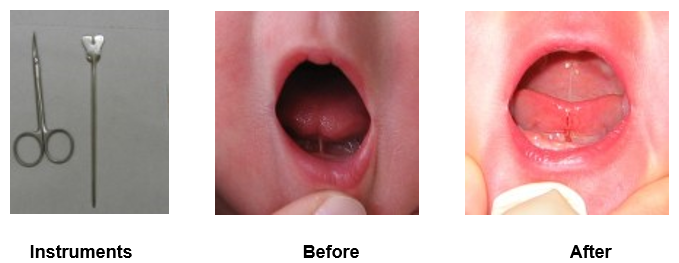
Once it has been determined that the frenulum is too short and the baby is not able to drink affectively from the breast, the problem can be solved with a simple procedure, namely cutting the frenulum. The sooner after the diagnosis it is done, the better.
The procedure
- The entire procedure takes less than 15 seconds and does not require anaesthesia. The frenulum is very thin and has few nerves, meaning there is very little pain associated with the procedure
- The baby may cry because the nurse should keep the baby’s head and arms still and his lower jaw low
- Sometimes there is a little drop of blood visible
- Before and after the frenotomy the baby can be restless, a few drops of sucrose water will comfort the baby
- Immediately after the frenotomy you can breastfeed your baby again
In some cases, the frenulum is thick and fleshy. Then a frenotomy will not be enough and a frenectomy will have to take place to loosen the tongue. This procedure, where (a part of) the frenulum will be cut out and the wound will be stitched, is done under anaesthesia. Therefore the doctor will refer you to an ENT-specialist or a dental surgeon.
Frenotomy in the Reinier de Graaf Hospital
In the hospital, there is a neonatologist who can perform the procedure. In the absence of one, you will be referred to an ENT specialist.
In principle, only tongue ties of type 1 and 2 are divided. The reasons for this:
In the obstetrician department
Bij posterior tongriem type 3 of 4 is de opnameduur te kort om te kunnen beoordelen of gekliefd moet worden. Aanlegtechnieken dienen eerst verbeterd te worden.
The length of stay in the hospital is too short to observe if frenotomy of a posterior tongue tie type 3 or 4 is necessary. Breastfeeding techniques must first be improved.
In the neonatology department
In case of a posterior tongue-tie type 3 or 4 it’s important to consider whether frenotomy will yield such a result that this sufficiently outweighs the risk of developing food refusal due to the negative experiences in the mouth area during and after cleaving. This is especially important in the young preterm infants.
Healing of the wound
Within 24 hours of wound creation, the edges of the wound begin to migrate towards the centre of the wound so that the edges can try and eventually zipper together with a mucous membrane covering. This migration is facilitated by a scaffolding that forms over the wound (this is the white/yellow colour we see as an oral wound is healing.
Exercises for tongue/mouth after frenotomy are important!
- To let your baby get used to the new mobility of the tongue
- To improve the muscle power and coordination of the tongue
Massage to prevent the tongue tie from growing together again
The massage should always be done after the procedure. It is best to start on the day of the procedure, 3 times each day, for a minimum of 3 days:
- Wash your hands
- Lift up the tongue carefully with your fingertips on both sides of the frenulum
- Massage with the tip of your finger the centre of the small wound in small circles for a few seconds
Instruction video for massage:
https://youtu.be/2JMcbF85ehs When improvement during breastfeeding is seen immediately after the procedure, no further tongue exercises are necessary accept the massage. The drinking itself is enough practice for your baby.
Other exercises
If the mobility of the tongue is still not optimal, do the exercises listed below with your baby.
Wash your hands first.
- Muscle relaxation exercises
- Slowly massage with your fingertips baby’s cheeks by making round movements
- Then rub your finger around the mouth, and massage the lips. This will relaxes the jaws.
- Tug-of-war with the thumb
- Let the baby suck on your thumb (fingernail on the tongue), and while sucking let the thumb sink deeper into the mouth to about 4 cm
- Gently pull back your thumb a few millimetres, if your baby is sucking hard. This is to encourage the baby to hold the thumb firmly with his tongue.
- Stick out the tongue
- Touch with a finger (with a little milk) the upper or lower lip and/or the jaw edges, to lure the tongue out of the mouth
- Run your finger back and forth over the jaw edge, to provoke the tongue to move sideways
- Mirroring
- Hold your baby 20-30 cm in front of your face. Stick out your own tongue and make an ‘aaaahh’ sound. The baby will mirror your movement and stick out his tongue as well
- Wiggling
- Let your baby suck on your finger, turn your finger around (fingernail towards the roof of the mouth) and wiggle/walk your finger out of the mouth, while keeping a little pressure on the tongue. The purpose of this is to stimulate the tongue to move more and to cup around your thumb
- Mouth game
- You can elaborate the exercises above by turning them into games.
- Watch the instruction video: https://youtu.be/fbGJvCR9nYM
For further information
Document NVL “Tong en lipriemen” on
www.nvlborstvoeding.nl.
Important telephone numbers
Reinier de Graaf Gasthuis 015 - 260 30 60
Maternity ward 015 - 260 35 35
Urgency or discomfort during pregnancy 015 - 260 33 30
Start of labor 015 - 260 32 30


 Favoriet
Favoriet Stuur door
Stuur door