An induction of labor helps to get the birthing process going. An induction (or the start of an induction) takes place in the hospital under the responsibility of a gynaecologist. This folder provides general information.Reasons to induce labor
If the gynaecologist in accordance with you has decided that it is better for your child to be born and not to remain in the womb any longer, labor will be induced. This happens at a time when your child is still in good condition and it is expected that the baby can withstand a normal delivery. Some common reasons for an induction are: being overdue, prolonged rupture of membranes, high blood pressure, fetal growth restriction and a deterioration of the functioning of the
placenta. Serious complaints from yourself, either physical or psychological, can also be a reason to induce labour. Sometimes the pregnant woman wants an induction herself, without there being any medical reason for this. The pros and cons of this should be carefully reviewed beforehand.
How to induce labor
There are three methods for inducing labour:
- placing a small balloon (“Foley catheter”) in the cervix;
- taking oral medication;
- breaking the membranes and starting an intravenous infusion.
Which method is used depends, among other things, on the cervix ripening. This means that it is checked to what extent your cervix has already softened and has expired, or whether it is dilated to allow breaking of the membranes. The doctor or hospital midwife will decide after an internal examination which method is most suitable in your situation. Regardless of the method of induction, a
cardiotocogram (
CTG) is taken before initiating induction. By means of two sensors on your abdomen, the heart rate of your child and the tension of the
uterus are registered.
Preparation
When you are scheduled for an induction, you should bring the same items with you as with a 'normal' birth: clothes for yourself for before, during and after labor, toiletries and baby clothes. It is also wise to bring something to relax and pass time. Inducing labor can sometimes take several days. Distraction can then be enjoyable.
Admission in the induction room
You will be admitted to a double room where a
CTG is taken. The internal examination and, if necessary the placement of a foley catheter, will take place in an examination room. Depending on the reason for the induction of your labor, you may then go home or remain admitted to the obstetrics department. If there is room, you can spend the night in the delivery room or the maternity room. In that case, your partner may stay overnight.
Induction with a foley catheter
The balloon catheter has several effects:
- The balloon stimulates the release of natural hormones that cause the cervix to ripen.
- The balloon gives pressure, which causes dilation of the cervix.
Method
- You take a seat in the gynaecological chair, after which the doctor or hospital midwife performs a vaginal examination. After this, a speculum is inserted or, when possible, the procedure is followed without a speculum.
- A tube with an inflatable balloon (“foley catheter”) is inserted into the uterus, just above the cervix. The balloon at the end is inflated with a small amount (50 mL) of water. After insertion, an internal examination or an internal ultrasound is used to check whether the catheter is in the right place. The catheter exits through the vagina and is taped to your thigh.
- After the balloon has been placed, you can return to your room where another CTG will be made for one hour.
Placement of a foley catheter can feel uncomfortable. You can still go to the toilet or shower. If the plaster with which the catheter is attached to your leg comes loose, you can simply stick it again.
You may have some vaginal bleeding after insertion of the balloon catheter. This is mostly innocent. It is also possible to experience uterine contractions or “Braxton Hicks contractions”. Sometimes these Braxton Hicks evolve to contractions that cause cervical dilatation. Depending on the reason for the induction, you will remain hospitalized or you may go home afterwards. This also depends on your condition and wishes and the condition of your child.
When you go home you will receive more information when to contact us and when we expect you to be back in the hospital.
The morning after placement of the foley catheter will be checked whether the balloon has already come through the cervix. An internal examination is performed again. Depending on the examination, the balloon may be left in place or a new one is inserted. Also, the method of induction may be switched to oral medication. If the desired result has not yet been achieved after a few days, the gynaecologist will discuss further policy with you.
If you are allergic to latex, it is important to let us know in advance. In that case, a latex-free balloon catheter is used.Induction with hormones
Sometimes induction with a balloon catheter is not suitable for you or it does not have the desired effect. Another option is to induce labor with Misoprostol (Angusta). These are tablets that contain prostaglandins. Prostaglandins are hormones that ripen the cervix. Prior to induction with Angusta, the child’s condition is observed by a
CTG. In addition, an internal examination is performed. This may be sensitive. After the examination you can then take the provided tablet(s) with a sip of water. Then another
CTG examination will take place for at least an hour.
Every four hours, the doctor or midwife assesses whether more Angusta is needed. This depends on the contractions you experience and whether the cervix has ripened. An internal examination will then be performed again. Misoprostol is administered up to four times in one day. An induction with Angusta requires hospitalization.
Breaking membranes
If the cervix feels ripe and there is sufficient cervical dilation, it is possible to continue the induction by rupturing the membranes. An infusion will be inserted into your lower arm or hand. Through the IV, synthetic oxytocin (Syntocinon) is administered to initiate contractions. The dose increases step-by-step. Depending on the contractions you experience, the opening of cervix and the condition of the child the dose may or may not be raised.
During induction and labor
Your child's condition will be checked using a
CTG. This can be done externally with a sensor on the abdomen, or internally through a wire (scalp electrode) on the child's head. The contractions are measured through a sensor on the abdomen.
After induction with Syntocinon started, labor will continue the same as a 'normal' birth. The contractions gradually become more intense and painful. In general, you can handle the contractions in the way you prefer: sitting in a chair, standing next to the bed, on a yoga ball and lying or sitting in bed. The birth of the child and the
placenta are no different than with a 'normal' birth. Your baby will generally be born within 24 hours after the membranes are ruptured.
Caregivers
During a medical birth, you will be accompanied by a hospital midwife and/or doctor. They work in close collaboration and under the responsibility of the gynaecologist and will consult the gynaecologist at any moment if necessary. Also, an obstetric nurse or maternity care provider will be present at the birth. In addition, there are also student nurses, student midwives or interns (medical students). It will be discussed with you in advance whether they can be present.
After birth
After the birth, the doctor, hospital midwife or pediatrician will check your childs condition. About two hours after the birth of the
placenta, the nurse removes the IV. If the delivery goes well and no further check-ups are necessary, you can go home a few hours after the delivery. Sometimes the advice is to stay longer, if longer observation of or more
care for either you or your child is needed.
Important telephone numbers
Reinier de Graaf Gasthuis 015 - 260 30 60
Maternity ward 015 - 260 35 35
Urgency or discomfort during pregnancy 015 - 260 33 30
Start of labor 015 - 260 32 30
For more information
https://reinierdegraaf.nl/inleiden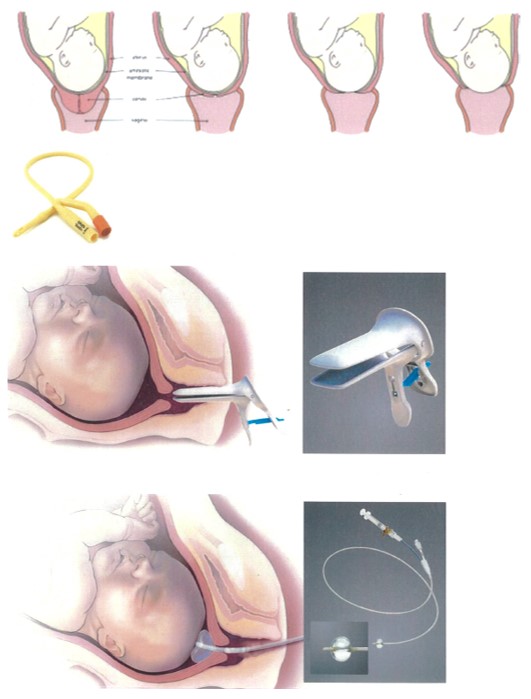


 Favoriet
Favoriet Stuur door
Stuur door